Diagnosis
Hemophilia is diagnosed by extracting a sample of blood from the patient and testing the blood for adequate levels of clotting factors. Diagnoses can occur during the fetal stage as well; some parents who carry the hemophilia gene choose to have a prenatal diagnosis only if ultrasound reveals that the child will be male, as males have a much higher risk of having hemophilia. Prenatal testing is covered by health insurance for most Canadians.
Hemophilia is diagnosed by extracting a sample of blood from the patient and testing the blood for adequate levels of clotting factors. Diagnoses can occur during the fetal stage as well; some parents who carry the hemophilia gene choose to have a prenatal diagnosis only if ultrasound reveals that the child will be male, as males have a much higher risk of having hemophilia. Prenatal testing is covered by health insurance for most Canadians.
Treatment
There is currently no cure for hemophilia, though life expectancies of hemophiliacs are rising due to better treatment. Mild hemophiliacs usually do not require treatment though sometimes a hormone called desmopressin is given to those with mild hemophilia A. Desmopressin causes a rise in factor VIII and the Von Willebrand factor in the blood.
There is currently no cure for hemophilia, though life expectancies of hemophiliacs are rising due to better treatment. Mild hemophiliacs usually do not require treatment though sometimes a hormone called desmopressin is given to those with mild hemophilia A. Desmopressin causes a rise in factor VIII and the Von Willebrand factor in the blood.


Replacement Therapy
This is the most common form of treatment for hemophilia. When used to prevent excessive bleeding, it is called preventive or prophylactic treatment; when used on an as-needed basis, it is called demand therapy.
Essentially, the missing clotting factor is dripped or injected into a vein. The clotting factor concentrates can be distilled from human blood. Though the risk of getting diseases transmitted through blood is very small due to screening and treatment of the blood before using, “recombinant” clotting factors are also available. These factors are usually cultured in animal tissues. This treatment may be used as regularly as a couple of times per week, to prevent spontaneous bleeding episodes for severe hemophiliacs, or before, during or after a surgical treatment for moderate hemophiliacs. Mild hemophilia rarely needs to be treated with replacement therapy.
In 20-30% of hemophilia A cases and 2-5% of hemophilia B cases, the body develops antibodies, called inhibitors, that destroy clotting factors from replacement therapy before they can become effective. This is a serious problem, as the body is attacking proteins that it needs. Doctors may try larger doses of factors, or use factors gathered from different sources. Recombinant factor VII may partially solve the problem. Researchers are looking for other ways to deal with these inhibitors.
(photo above shows a commercially produced vial of Advate, recombinant factor VIII. It is to be mixed with water and used for replacement therapy).
This is the most common form of treatment for hemophilia. When used to prevent excessive bleeding, it is called preventive or prophylactic treatment; when used on an as-needed basis, it is called demand therapy.
Essentially, the missing clotting factor is dripped or injected into a vein. The clotting factor concentrates can be distilled from human blood. Though the risk of getting diseases transmitted through blood is very small due to screening and treatment of the blood before using, “recombinant” clotting factors are also available. These factors are usually cultured in animal tissues. This treatment may be used as regularly as a couple of times per week, to prevent spontaneous bleeding episodes for severe hemophiliacs, or before, during or after a surgical treatment for moderate hemophiliacs. Mild hemophilia rarely needs to be treated with replacement therapy.
In 20-30% of hemophilia A cases and 2-5% of hemophilia B cases, the body develops antibodies, called inhibitors, that destroy clotting factors from replacement therapy before they can become effective. This is a serious problem, as the body is attacking proteins that it needs. Doctors may try larger doses of factors, or use factors gathered from different sources. Recombinant factor VII may partially solve the problem. Researchers are looking for other ways to deal with these inhibitors.
(photo above shows a commercially produced vial of Advate, recombinant factor VIII. It is to be mixed with water and used for replacement therapy).
Current Research: Gene Therapy
Gene therapy involves altering genes in those with severe hemophilia. Liver cells are usually altered or transplanted, to produce more of the clotting factors they are missing. This has cured hemophilia B in mice; in clinical trials in 2016, however, this form of treatment was only provided a short-term solution. Researchers hypothesize that the transplanted liver cells are attacked in the body, much like transplanted tissues are. Second rounds of clinical studies are underway, and are open to patient recruitment. Gene therapy is not a currently accepted form of treatment.
Gene therapy involves altering genes in those with severe hemophilia. Liver cells are usually altered or transplanted, to produce more of the clotting factors they are missing. This has cured hemophilia B in mice; in clinical trials in 2016, however, this form of treatment was only provided a short-term solution. Researchers hypothesize that the transplanted liver cells are attacked in the body, much like transplanted tissues are. Second rounds of clinical studies are underway, and are open to patient recruitment. Gene therapy is not a currently accepted form of treatment.
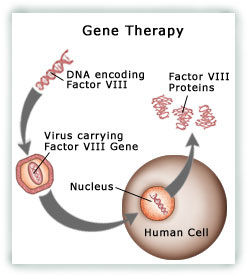
short explanations of gene therapy
|

|
